
Why OCD Is Underdiagnosed and Undertreated: Barriers to Care
How stigma, cost, and lack of specialists contribute to the OCD care crisis and what can help
Obsessive-Compulsive Disorder (OCD) is common, impairing, and highly treatable. Yet millions of people never receive the diagnosis or specialized treatment they need. Recent research from the International OCD Foundation highlights a stark reality: the U.S. is facing an “OCD care crisis,” marked by widespread underdiagnosis and limited access to evidence-based care.
This crisis disproportionately affects men and people of color, who often face unique cultural, systemic, and financial barriers when seeking help. Understanding these inequities is essential to improving access and outcomes—and to ensuring that effective treatments like Exposure and Response Prevention (ERP) reach those who need them most.
The OCD Care Crisis: A Gap Between Need and Access
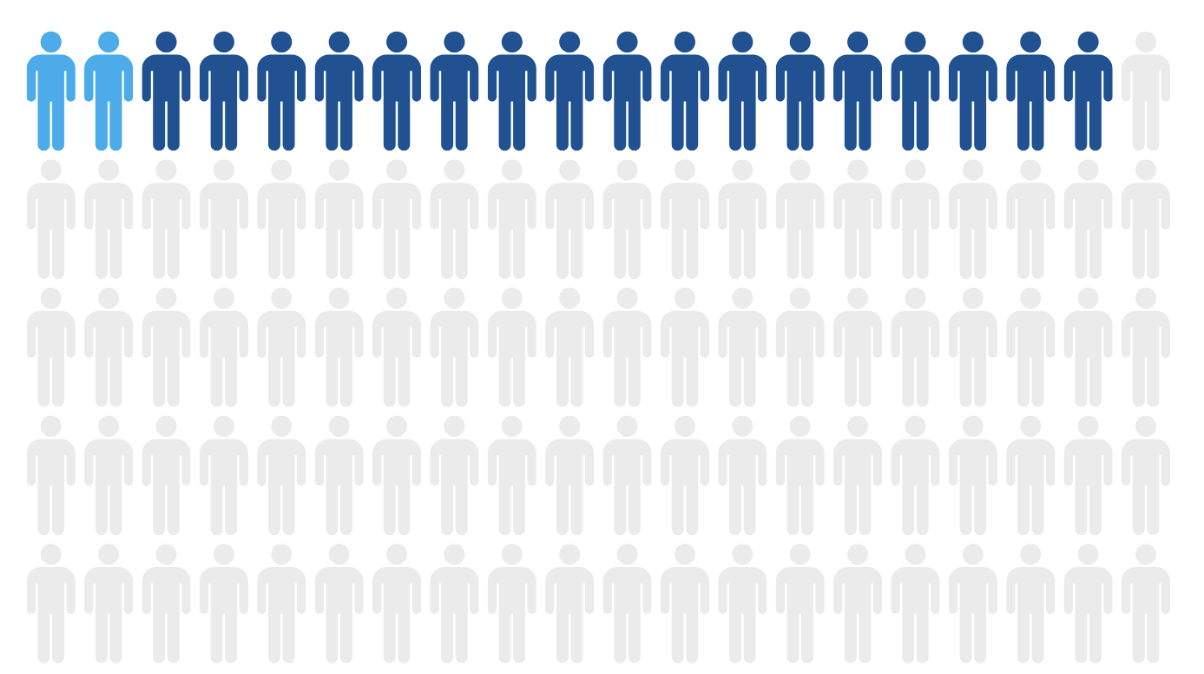
Research examining millions of electronic health records found that OCD is significantly underdiagnosed in clinical settings. Although lifetime prevalence is estimated at up to 3%, only about 0.51% of patients had a formal OCD diagnosis documented, suggesting that up to 75% of actual cases may go undetected.
Even more concerning is the treatment gap. While ERP is considered the gold-standard therapy for OCD, only 2% of patients had documented evidence of receiving ERP, and more than 80% did not receive recommended evidence-based treatment.
These findings reflect a systemic issue. Millions live with untreated OCD symptoms not because treatment does not exist, but because access to specialized care remains limited.
Why OCD Is Underdiagnosed in Men and People of Color
1. Cultural Stigma and Misconceptions
Many individuals delay seeking help due to stigma surrounding mental health. This stigma can be particularly strong in some cultural communities and among men, where emotional struggles may be minimized or reframed as personality traits rather than treatable conditions.
Obsessive thoughts and compulsive behaviors are often misunderstood or hidden due to shame, especially when symptoms involve taboo or intrusive content. This can lead to years of silent suffering before a person seeks professional evaluation.
Research shows that OCD is frequently mislabeled as generalized anxiety, depression, or personality traits, contributing to delayed diagnosis and treatment.
How stigma impacts help-seeking
Men may avoid treatment due to cultural expectations around self-reliance
Communities of color may face generational mistrust of healthcare systems
Religious or cultural interpretations of intrusive thoughts may delay clinical recognition
When symptoms remain concealed, clinicians may miss key diagnostic clues, reinforcing the cycle of underdiagnosis.
2. Cultural Barriers in Assessment and Diagnosis
Standard diagnostic tools may not fully account for culturally shaped expressions of OCD. For example, intrusive thoughts related to morality, contamination, or harm may be interpreted differently across cultures. Without culturally competent assessment, symptoms can be overlooked or mischaracterized.
Additionally, clinicians without specialized OCD training may not recognize subtle compulsions such as mental rituals, reassurance-seeking, or avoidance behaviors. This contributes to the finding that the majority of individuals with OCD never receive an accurate diagnosis.
Barriers to OCD Treatment: Cost, Insurance, and Lack of Specialists
1. The Shortage of OCD Specialists
Effective treatment for OCD requires specialized training in ERP. However, the IOCDF report indicates that many clinicians either do not provide ERP or fail to refer patients to specialists who do.
This creates a significant access bottleneck. Even when individuals are diagnosed, they may struggle to locate clinicians who offer evidence-based OCD treatment.
Consequences of limited specialization
Long waitlists for ERP-trained therapists
Geographic disparities in care availability
Clients receiving general therapy rather than OCD-specific treatment
Without specialized care, symptom improvement may be limited despite ongoing therapy.
2. Financial and Insurance Barriers
Cost is one of the most common obstacles to accessing OCD treatment. Specialized services are often out-of-network, and insurance plans may restrict session frequency or reimbursement rates for ERP.
This financial strain can lead individuals to delay or discontinue treatment, even when symptoms are severe. Global data also show that treatment access varies dramatically by economic resources, highlighting how financial barriers widen the care gap.
Common financial obstacles
High out-of-pocket costs for specialized ERP providers
Limited in-network options for OCD-focused therapy
Coverage restrictions for intensive or longer-term treatment
For many families, accessing effective OCD treatment becomes a logistical and financial challenge rather than a clinical one.
The Equity Gap: Why Access Matters
When stigma, misdiagnosis, cost, and specialist shortages intersect, certain populations are disproportionately affected. Men and people of color may face layered barriers that delay care for years.
Delayed treatment is not a minor issue. OCD symptoms can become more entrenched over time, affecting relationships, work, academic functioning, and overall quality of life. Fortunately, research shows that up to 80% of individuals improve significantly when they receive appropriate evidence-based treatment such as ERP.
This underscores a critical point: the problem is not a lack of effective treatments, but unequal access to them.
Bridging the Gap: Increasing Access to Specialized OCD Care
Addressing the OCD care crisis requires both systemic change and innovative service delivery models that remove common barriers.
Expanding Flexible and Specialized Care Options
At OCD & Anxiety Treatment of Houston (OATH), we are committed to addressing the disparities highlighted in national research. Our practice focuses exclusively on evidence-based treatment for OCD and anxiety disorders, using CBT, ERP, and ACT approaches tailored to each client’s needs. We also offer models of care to help reduce logistical and financial barriers while ensuring treatment fidelity to evidence-based protocols.
- In-network with Aetna insurance and offering reduced-rate individual and group therapy options to increase financial accessibility
- Telehealth therapy across Texas to reach underserved areas
- Intensive outpatient or structured ERP programs
- Culturally responsive and stigma-informed treatment approaches
- In-home ERP sessions for individuals unable to travel
We recognize that many clients come to us after years of being misunderstood, misdiagnosed, or unable to access specialized care. By offering flexible formats, including in-home sessions and virtual therapy across Texas, we aim to make high-quality OCD treatment more accessible to diverse communities.
Our mission is not only symptom reduction, but equitable access to specialized care that empowers clients to reclaim their lives.
Final Thoughts
The IOCDF’s findings make one thing clear: OCD is highly treatable, yet most individuals never receive the care they need. Underdiagnosis, stigma, financial barriers, and a shortage of specialists create a perfect storm that disproportionately affects men and people of color.
Improving access to culturally responsive, evidence-based OCD treatment is not just a clinical goal, it is an equity issue. By increasing awareness, expanding specialized services, and reducing systemic barriers, we can begin to close the treatment gap and ensure that effective care reaches everyone who needs it.
References
International OCD Foundation. (2025). America’s OCD Care Crisis.
International OCD Foundation. (2025). America’s OCD Care Crisis: Stories Behind the Statistics.
TherapyRoute. (2025). Obsessive-Compulsive Disorder (OCD) Statistics.